1. Regarding atomic structure:
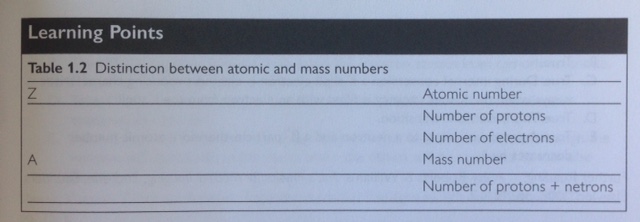
A. Z is the atomic number & indicates the number of protons in the nucleus
B. A is the mass number. Z determines place in the periodic table
C. Higher atomic number nuclei require more neutrons than protons for stability
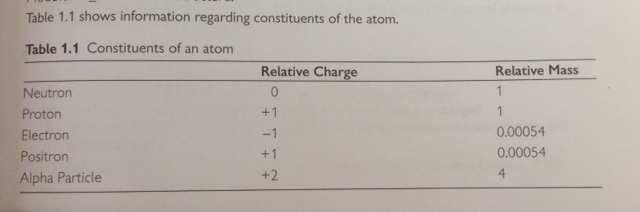
D. Neutrons have no charge, protons +1
E. They (Protons to neutrons in the nucleus) are tightly bound
2. Concerning orbital electrons
A. Electrons are arranged in shells around the nucleus at specific energy levels
B. Binding energy is expended completely removing the electron from the atom
C. It (Binding energy) is lowest for valence shell electrons and highest for the K shell
D. Characteristic radiation is from inner shells. The valence shell gives the chemical properties
E. K shell binding energy increases with increasing atomic number
3. Regarding the structure of atoms:
A. A proton has a mass approximately 1850x that of an electron
B. An electron is not a nucleon; Neutrons & Protons are nucleons
C. Positrons have the same mass as electrons
D. Alpha particles consists of 2 protons & 2 neutrons (helium nucleus), therefore the mass is 4x that a proton
E. There can be up to 2 electrons in the K shell, 8 in the L shell, 18 in the M shell and 32 in the N shell

4. Nuclides:
A. Each particular combination of Z and A defines a nuclide
B. Nuclides with the same number of protons but different number of neutrons are isotopes, therefore they have the same atomic numbers and different atomic mass
C. Not all are radioactive
D. Have the same chemical properties between isotopes of a particular element; Isotopes have the same number of protons and therefore when neutral the same number of electrons
E. May emit radiation if they have too few or too many neutrons

5. Regarding the electromagnetic spectrum
A. Sound waves do no fall within the spectrum
B. Frequency increases with energy, but velocity is constant
C. Frequency and wavelength of electromagnetic radiation are directly proportional to each other
D. All electromagnetic radiation travels at the speed of light in a vacuum; In a vacuum. velocity of radio waves is equal to that of infrared light.
E. UV light is further up the spectrum, therefore has a shorter wavelength than visible light.
6. Electromagnetic radiation:
A. Travels in straight lines if unattenuated
B. Have wave- & particle-like properties
C. Has energy that is usually expressed in electron volts (eV), which give manageable numbers for calculations (1eV = 1.6 x 10^-19Joules)
D. Comprises sinusoidally varying electric and magnetic fields perpendicular to each other & to the direction of travel
E. Does not include beta radiation; Beta particles are electrons emitted from the nucleus
7. Ionizing radiation:
A. Causes direct damage if it is absorbed in tissue
B. Causes indirect damage through ionisation of water & production of free radicals
C. Does not always obey the inverse square law; Only applicable to types of electromagnetic radiation from a point source and without attenuation
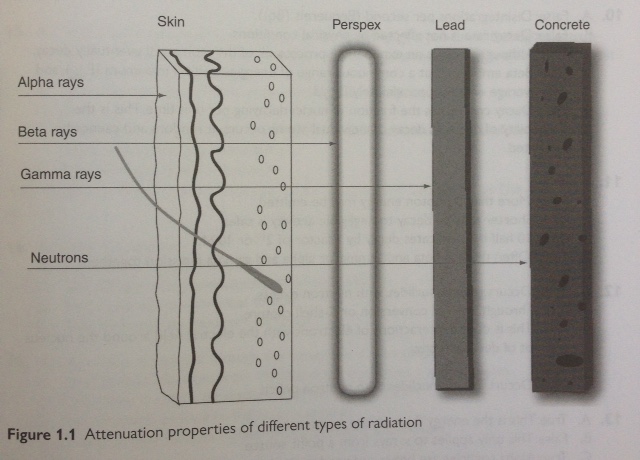
D. Gamma & X-rays are useful, neutrons, alpha, and beta particles are not
E. Beta radiation may require only Perspex shielding, however optimal shielding is achieved with Perspex backed with lead

8. Regarding secondary electrons:
A. They are recoil electrons produced during Compton scattering events
B. Their range depends upon the density of the material through which they are travelling & range also depends upon their initial energy
C. They interact with outer shell electrons to cause ionisation
D. They are the reason that x-ray and gamma rays are indirectly ionising; Alpha & beta particles are directly ionising as they are charged
E. Energy from the x-ray beam is converted into increased molecular motion & therefore heat.
9. In radioactive decay:
A. A neutron converts to a proton & a beta- particle, therefore atomic number increases by 1
B. Alpha particles are helium nuclei
C. Some radionuclides emit electrons and characteristic x-rays; During internal conversion a K shell electron is ejected, producing characteristic x-rays when the K shell vacancy is filled with an electron from the L shell.
D. Most nuclides left in the metastable state after beta decay, emit gamma rays to reach ground state; This is isometric transition
E. Positron emission reduces the number of protons in an atom by 1; A proton converts to a neutron and a beta+ particle, therefore atomic number decreases by 1
10. Regarding radioactivity:
A. Radioactive decay is the number of disintegrations per second (Bequerels (Bq))
B. Decay rate is not affected by physical conditions
C. If stored long enough, the radioactivity of a radionuclide will drop to zero; Although decay is an exponential process, all of the atoms will eventually decay.
D. Beta emission is at a continuous range of energies up to a maximum (Emax), and with average energy approximately Emax/3
E. Decay constant is the fraction of nuclei decaying per unit time. This is the probability of decay, as decay of individual atoms occurs at random and cannot be predicted.
11. The following are true of radionuclides:
A. Physical half-life (t1/2) is the time taken for the activity to decay to 1/2 the original value
B. Gamma rays are emitted at more than 1 photon energy
C. Gamma emitting radionuclides with shorter t1/2 are safer to use and store than thos with longer t1/2; Shorter time to decay to negligible activity is safer
D. In 10 half-lives the activity is reduced by a factor of approximately 1000; 10 half lives indicates decay by a factor of 2^10 or 1024
E. Often there is beta & gamma, or alpha & gamma emission together
12. Direct emission from radioactive decay includes:
A. Beta minus emission; Occurs in radionuclides with neutron excess
B. Characteristic x-rays; Through internal conversion or K-shell capture
C. Bremsstrahlung is due to interactions of electrons with the electric field around the nucleus and not of decay directly.
D. Alpha particles
E. Positron emission; Occurs in radionuclides with neutron deficit
13. Concerning properties of x-rays:
A. Beam intenstiy is the total energy per unit area per unit time; This is the energy fluence rate or intensity
B. The inverse square law applies to x-rays from a point source
C. X-rays have lower linear energy transfer than alpha particles; Alpha particles are heavy & produce ionizing events closely spaced along a short path, causing maximum DNA damage.
D. Only high-energy photons (x-rays/ gamma rays) are ionizing
E. At equivalent energy, an x-ray cannot be distinguished from a gamma ray; How they are produced differs, but they are indistinguishable at equivalent energies.